Peptide Combinations Guide
Growth Hormone (GH) and IGF-1 are naturally occurring hormones in the human body responsible for many enviable aesthetic traits such as muscle mass, leanness and a firm/even skin tone. As people age, levels of growth hormone rapidly decline and this is one of the main reasons humans put on weight, lose muscle mass and develop sagging/uneven skin. It's no surprise then that synthetic Human Growth Hormone is a sought after product for anti-aging by persons looking to remain youthful, bodybuilders looking to put on muscle mass and people in general who are looking to "tone up" or lose stubborn belly fat.
It is important to note that the products mentioned on this website are not the actual synthetic HGH (although HGH Frag 176-191 is the part of the "real" HGH which contributes to fat loss only). But in many respects these peptide analogues are far superior to the HGH 191aa drug for 3 reasons:
Actual HGH is very difficult or impossible to obtain in most countries and is one of the most faked/counterfeit drugs sold online.
If HGH can be obtained legally from a physician for anti-aging it's extremely expensive, with 10iu (units) costing as much as $200USD. As a comparison, the 10iu equivalent of GH releasing peptides (approximately half of one vial) sells online for approximately $20USD, a full 90% cheaper than actual HGH for the same, if not better, positive effects on the body.
Since actual HGH shuts down the body's natural pituitary gland, when you stop injecting it, your body's own ability to produce Growth Hormone is hindered and you will suffer a rebound of negative side effects such as fat gain, muscle loss and loss of skin tone/elasticity. This means you may end up doing yourself more harm than good. Since GH releasing peptides only stimulate your body's own natural production, there is no rebound negative effects if you stop usage.
The following guide indicates the best way to combine different peptides depending on your experience level of diet/training and also your goal:
Fat Loss
Muscle Building
Anti-Aging
As a general introduction, you should understand the different classes of peptides as this largely determines their combinations:
Growth Hormone Releasing Hormones (GHRH): include Modified GRF 1-29 and CJC-1295 DAC, are peptides which stimulate the pituitary gland to release stores of the body's natural Growth Hormone (GH).
Growth Hormone Releasing Peptides (GHRP): include Ipamorelin, GHRP-2 and GHRP-6, peptides which stimulate the release of a hormone called "Ghrelin" in the stomach, which then in turn causes GH to be released. GHRP's cause a much more significant release of GH than do GHRH, meaning that mg for mg, a peptide like GHRP-6 is three times more potent than Modified GRF 1-29. However, when taken together, they become approximately ten times more potent than either one alone.
IGF-1 Peptides: include IGF-1 LR3 and IGF-1e (also known as MGF or Mechano Growth Factor). IGF-1 is responsible for many of the positive effects of GH on fat loss and muscle building therefore they offer a good addition, especially if your goal is to build muscle, as they are both responsible for creating new muscle cells which can hypertrophy (get bigger) through weight training.
HGH Fragment 176-191: is a peptide which does not stimulate the release of GH but is instead a piece (or "fragment") of the full synthetic 191aa HGH molecule. More importantly, it is the fragment of GH which is responsible for fat loss, meaning it gives all of the fat loss benefits without any side effects.
As a general rule, regardless of your goal, if you are just looking to take one product, with the least amount of fuss and injections as possible, then it should be CJC-1295 DAC at 2mg (1 vial) per week. Due to its long half-life it causes your overall level of GH (Growth Hormone) to rise, and you will therefore see some improvements in things which go along with having higher levels of GH and IGF-1 such as improved body shape, sleep, skin and general wellbeing (although it can make you tired for the first 1-2 weeks while the body adjusts). Your dosage can be taken as just one injection per week (note that you may notice a head rush/flushing for 15-20 minutes after your injection due to the release of GABA in the body, a sign the product is working).
For information about more intricate and advanced usage of GH peptides please read on.
Fat Loss
The most potent weight loss peptide is HGH Fragment 176-191 which is the part of the Growth Hormone molecule responsible for fat burning. In HGH Frag Studies, it has been proven to reduce body fat, particularly in the abdominal area. The second most potent fat loss peptide is CJC-1295 DAC since it causes the overall GH level to rise in the body (the opposite of what happens naturally as a person gets older, which is why people tend to put on weight as they age). If your only goal is fat loss, it's often best to avoid the use of GHRP products (GHRP-6, GHRP-2 or Ipamorelin) since they can stimulate hunger and/or raise cortisol, both of which can be counterproductive to fat burning.
Diet Considerations
For GH to exhibit its fat burning effects, insulin must NOT be present. Insulin release in the body is caused mainly by consuming carbohydrates, although all types of macronutrients (carbs, fat and protein) still cause the release of insulin to some extent. Since HGH Frag works by causing the body to break down and release stored fat for use as energy, if you have recently consumed calories (food or beverage) your body will just use that for energy instead and little extra fat will be burnt. If however there is no food present for the body to use as energy, it will use the stored fat which the HGH Frag has caused to be released and you will notice reductions in body fat over the ensuing weeks.
Due to CJC-1295 DAC's long half-life the timing of meals is not important and this is what makes it an appealing addition to HGH Frag 176-191 to accelerate fat loss. To get the most out of your peptide usage for fat loss, the following guidelines should be followed:
Avoid eating/drinking anything with calories for three (3) hours either side of your injection.
Try to make all your meals throughout the day high protein, low fat and low carbohydrates (eg. meat/fish with vegetables/salad).
Have as few meals as possible during the day as periods of fasting have been shown in many studies to improve fat loss and also longevity (i.e. eating less will make you live longer).
Sample Peptide Cycles
Beginners
HGH Frag 176-191 at 250-500mcg per day.
Advanced
HGH Frag 176-191 at 250-500mcg per day + CJC-1295 DAC at 300mcg per day or;
HGH Frag 176-191 at 250-500mcg per day + Modified GRF 1-29 at 100-300mcg per day (split into dosages of 100mcg)
Example Injection Routines
Example 1 - Night Time Injection (recommended)
Ensure you do not eat or drink anything containing calories within three (3) hours of going to bed (with the exception of water, diet sodas, coffee/tea with artificial sweeteners).
Take your HGH Frag 176-191 injection just before getting into bed and your body will therefore be burning stored fat for the duration of your sleep.
If possible, do some cardio first thing in the morning and wait as long as possible before having breakfast to allow the fat burning to continue throughout the morning/day.
Example 2 - Morning Injection
Wake up and inject your HGH Frag 176-191 (250mcg to 500mcg is a good dosage depending on your budget).
Wait as long as possible before having your first meal (the longer you wait the more fat you will burn).
When you do eat, try to make the meal high protein, low fat and low carbohydrate (example meat and salad/vegetables).
If possible, try to do some cardio in the hours after your injection to increase the fat burning effect.
Note: If you are a person concerned about loss of muscle mass, you can consume a small amount of protein every 2-3 hours (amino acid tablets such as EAA and BCAA are good for this purpose and can be purchased from any health food shop or ordered online). However there is little reason to be concerned about muscle loss because when fat is available for energy, such as following HGH Frag 176-191 injections, protein and therefore muscle mass are spared.
Adding CJC-1295 DAC
You can add CJC-1295 DAC at 2mg once per week (or 300mcg each day along with your HGH Frag 176-191 injections - they can be mixed in the same syringe without any issues). You should take a break from CJC-1295 DAC every few months to give your pituitary gland a rest at which time you can continue to use HGH Frag 176-191 on its own, or you can substitute the CJC-1295 DAC with the short acting Modified GRF 1-29 at 100-300mcg per day (split into injections of 100mcg).
Muscle Building
Growth Hormone (GH) exhibits its muscle building effects mainly after its conversion to IGF-1 (Insulin-Like-Growth Factor). This makes IGF-1 an ideal choice of peptides for muscle building, especially since the IGF-1 LR3 version has an extended half-life which allows it to remain active in the muscles for many hours to complete its muscle building stimulatory effects. Likewise, if injected after a workout, the IGF-1 variant Mechano Growth Factor (also known as MGF or IGF-1e) is known to multiply muscle cells and contribute to muscle development. Furthermore, since IGF-1 is a by-product of GH, any peptide which increases levels of GH in the body such as a GHRP product or CJC-1295 product will obviously lead to increased lean muscle mass.
Diet Considerations
For Growth Hormone (GH) to perform its anabolic (muscle building) affects it requires the presence of the body's most anabolic hormone: insulin. This is in contrast to GH related fat loss which requires insulin to be absent. However, since GHRP and fast-acting GHRH (Growth Hormone Releasing Hormone) products (i.e. Modified GRF 1-29) still need time to stimulate the body to release GH from the pituitary gland, the insulin spike must come after the injection and not before, otherwise the GH release will be blunted.
The only exception to this is of course CJC-1295 DAC since it's long-half life and continual release of GH means it is not affected by food timing.
To get the most out of your peptide usage for muscle building, the following guidelines should be followed:
If injecting just a GHRP or GHRH product on their own, avoid eating/drinking anything high in fat for 3 hours before your injection and anything high in carbohydrates for 2 hours before (i.e. always do your injection on an empty stomach), otherwise the amount of GH release they cause may be significantly blunted leading to poor results.
If injecting both a GHRP and GHRH together (e.g. 100mcg of both GHRP-6 and Modified GRF 1-29) studies have proven that their ability to release GH returns to full-strength as little as 1 hour (60 minutes) post-meal. This gives users greater flexibility with their meal timings, especially since consuming sufficient calories is so critical to building muscle.
Whether injecting GH peptides alone or along with others, always wait at least 20 minutes after your injection before consuming anything. Once at least 20 minutes has passed, consume a food/beverage high in protein and/or carbohydrates to stimulate an insulin spike (if you inject in the morning and around your workout, this meal/shake should be high protein and high carbohydrates, if you inject at night this consumption should be protein only as protein is sufficient enough to spike insulin, but without the negative impact on fat gain which carbohydrates can contribute to).
Sample Peptide Cycles
Beginners
CJC-1295 DAC at 2mg per week or;
GHRP Product (GHRP-6, GHRP-2 or Ipamorelin) at 200mcg once per day.
Intermediate
GHRP Product at 200mcg + Mod. GRF 1-29 at 100mcg (2 times per day) or;
GHRP Product at 200mcg + CJC-1295 DAC at 100mcg per day (2 times per day).
Advanced
GHRP Product at 200mcg + CJC-1295 DAC at 100mcg (2 times per day) + IGF-1 at 50mcg after workouts or;
GHRP Product at 200mcg + Mod. GRF 1-29 at 100mcg (2 times per day) + PEG-MGF at 200mcg after workouts.
Example Injection Routines
Beginners
CJC-1295 DAC
2mg taken once per week, at any time of day.
GHRP + GHRH (once per day)
Inject your dosage (ensuring you have not consumed any food/beverages for at least 1 hour before, an optimal time would be first thing in the morning).
Ingest a protein only or protein and carbohydrate meal afterward to create an insulin spike.
Do weight training in the hours afterwards.
Intermediate
GHRP + GHRH (twice per day)
Inject your GHRP + GHRH peptides together in the same syringe (ensuring you have not consumed any food/beverages for at least 1 hour before, an optimal time would be first thing in the morning).
Ingest a protein only or protein and carbohydrate meal afterward to create an insulin spike.
Do weight training in the hours afterwards.
at least 1 hour after your dinner (or last meal of the day), take your second GHRP + GHRH injection.
If you are trying to control your body fat then have a protein only meal 20-30 minutes afterwards, otherwise a protein/carbohydrate meal will create a better insulin spike.
Advanced
GHRP + GHRH + IGF-1
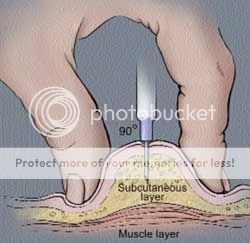
Follow the same routine as shown above for "intermediate" persons. However, as soon as possible after your weight training you should also inject 200mcg of PEG-MGF (IGF-1e) and/or 50mcg of IGF-1 LR3 preferably into a muscle (although due to the long half-life of both products, sub-q injections are also acceptable). If injecting intramuscularly, you should make sure that the muscle you are injecting into is not covered by a thick layer of fat. Usually due to the length of insulin syringe needles, injections are therefore limited to the biceps for most persons.
While GHRP + GHRH can be injected each day with great benefit, even if you don't do weight training on that day. On the other hand, IGF-1 LR3 and MGF injections should be reserved for post-workout only.
Anti-Aging
For the Anti-Aging crowd, we recommend choosing only 1 peptide, rather than a combination. The reason for this is that as you get older your GH levels decline rapidly and therefore you will benefit from any kind of GH increase meaning there is no need to overdo things with multiple peptides. If you wish to use more than one peptide, we recommend cycling a GHRP product (GHRP-6, GHRP-2 or Ipamorelin) every 3-6 months with CJC-1295 DAC for two reasons.
The first reason is that CJC-1295 DAC is a GHRH (growth hormone releasing hormone) acting directly at the pituitary, while GHRP products indirectly stimulate GH by causing the release of Ghrelin. Rotating the products would therefore ensure one method of GH stimulation does not get "worn out" from repeated exposure to the peptides. The second reason is that even though CJC-1295 DAC has been proven safe in much higher dosages than we recommend, since it causes a continual GH release (GH bleed) no one can be certain how continual use would affect the pituitary in the long-term, so it's a case of being "better safe than sorry" and never using it for longer than 6 months at a time without a break.
Diet Considerations
For CJC-1295 DAC there are no particular diet restrictions that need to be followed due to its long half-life. For GHRP products the following should be observed as insulin and fatty acids can blunt the release of GH in the body and therefore make your injections less effective:
Avoid eating/drinking anything high in fat for 3 hours before your injection and anything high in carbohydrates for 1-2 hours (always do your injection on an empty stomach).
Wait at least 20 minutes after your injection before eating/drinking anything with calories.
Injection Amounts
CJC-1295 DAC taken at 2000mcg (2mg) once per week or;
GHRP Product (GHRP-2, GHRP-6 or Ipamorelin) taken at 200mcg per day.
Example Injection Routines
CJC-1295 DAC
2mg taken once per week, at any time of day.
GHRP-2, GHRP-6 or Ipamorelin
Example 1 - Night Time Injection (recommended to reduce possible tiredness during day).
Ensure you have an empty stomach (i.e. 2-3 hours since your last meal).
Inject your GHRP peptide and go straight to bed.
Example 2 - Morning injection
Take your injection of the GHRP product first thing in the morning at 100mcg.
Wait at least 20 minutes before having breakfast or any beverages (including coffee/tea).
(All info gathered via internet)